
What Your PPO Network Was Actually Designed to Do
When employers shop for health coverage, the conversation almost always begins with the same question: which network? The assumption embedded in that question is significant. It treats the network as the foundation of the benefits strategy—the starting point from which everything else is built. That assumption is worth examining.

In This Article
Preferred provider organization (PPO) networks were introduced in the early 1980s to solve a specific problem: how to give employees access to a broad range of providers while creating some structure around how claims were paid. The original design was straightforward: a network of hospitals and physicians agreed to accept patients covered by a given plan, and in exchange those doctors and facilities received a predictable flow of patients. Employers and insurers got a defined group of providers they could direct their employees toward. In other words, networks were designed to manage access. That was the whole job. And for a long time, they did that job reasonably well.
But, somewhere along the way, the network became something more than infrastructure. It became the strategy.
Access and cost control are not the same thing
Managing access to providers and controlling the cost of care are two different problems. Networks were built to solve the first one. They were never designed to solve the second. This distinction matters because most employer health plan conversations conflate the two. When an advisor presents a network, the implicit message is that the network is doing the work of cost management. Employers are shown large provider counts, geographic coverage maps, and discount percentages—all signals of a network’s reach and negotiating position.
But broad access does not guarantee cost discipline. A network can include thousands of providers across every major city while doing nothing to address whether those providers are billing at rational prices. The size of the network and the quality of its pricing are separate questions entirely.
Research consistently confirms this gap. A 2024 analysis published in Health Affairs Scholar found that hospital prices have risen steadily for nearly two decades—faster than insurance premiums or professional services—suggesting that network contracting has not been sufficient to contain the primary driver of healthcare costs.
Meanwhile, Mercer’s 2025 National Survey of Employer-Sponsored Health Plans found that the average cost of employer-sponsored health insurance reached $17,496 per employee—a 6% increase over the prior year, and part of a sustained period of elevated growth. Employers operating within traditional PPO network structures have largely absorbed these increases year after year. The network did not prevent those increases. It was not designed to.
The access promise is shakier than it appears
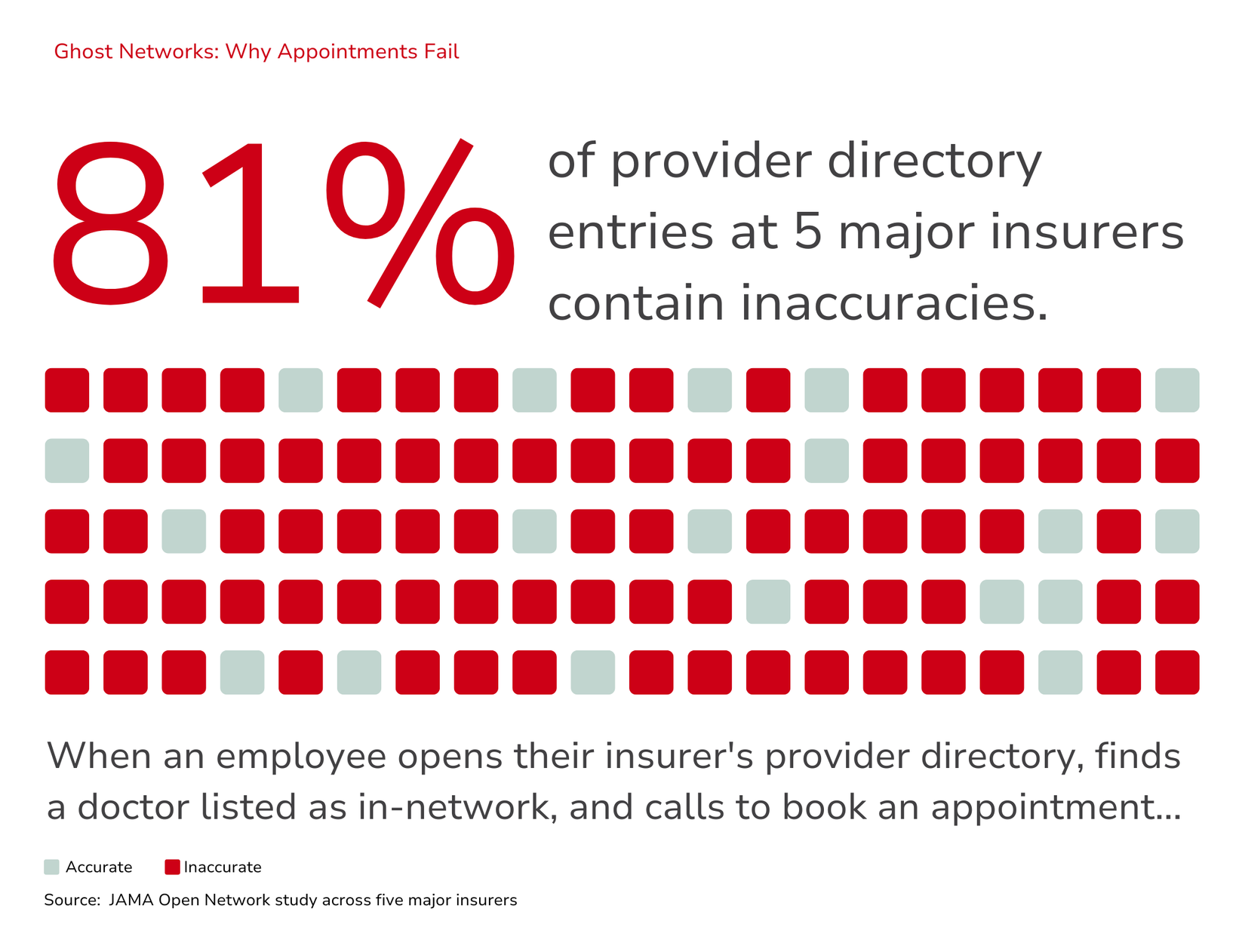
Even on its own terms—pure access—the network model has significant limitations that are not always visible to employers. Provider directories, the tool employers and employees rely on to understand who is in their network, are frequently inaccurate. This problem is widespread enough that researchers and regulators have given it a name: ghost networks. These are providers listed as in-network who are, in practice, unavailable. They are either not accepting new patients, no longer listed at the location, or no longer contracted with the plan at all.
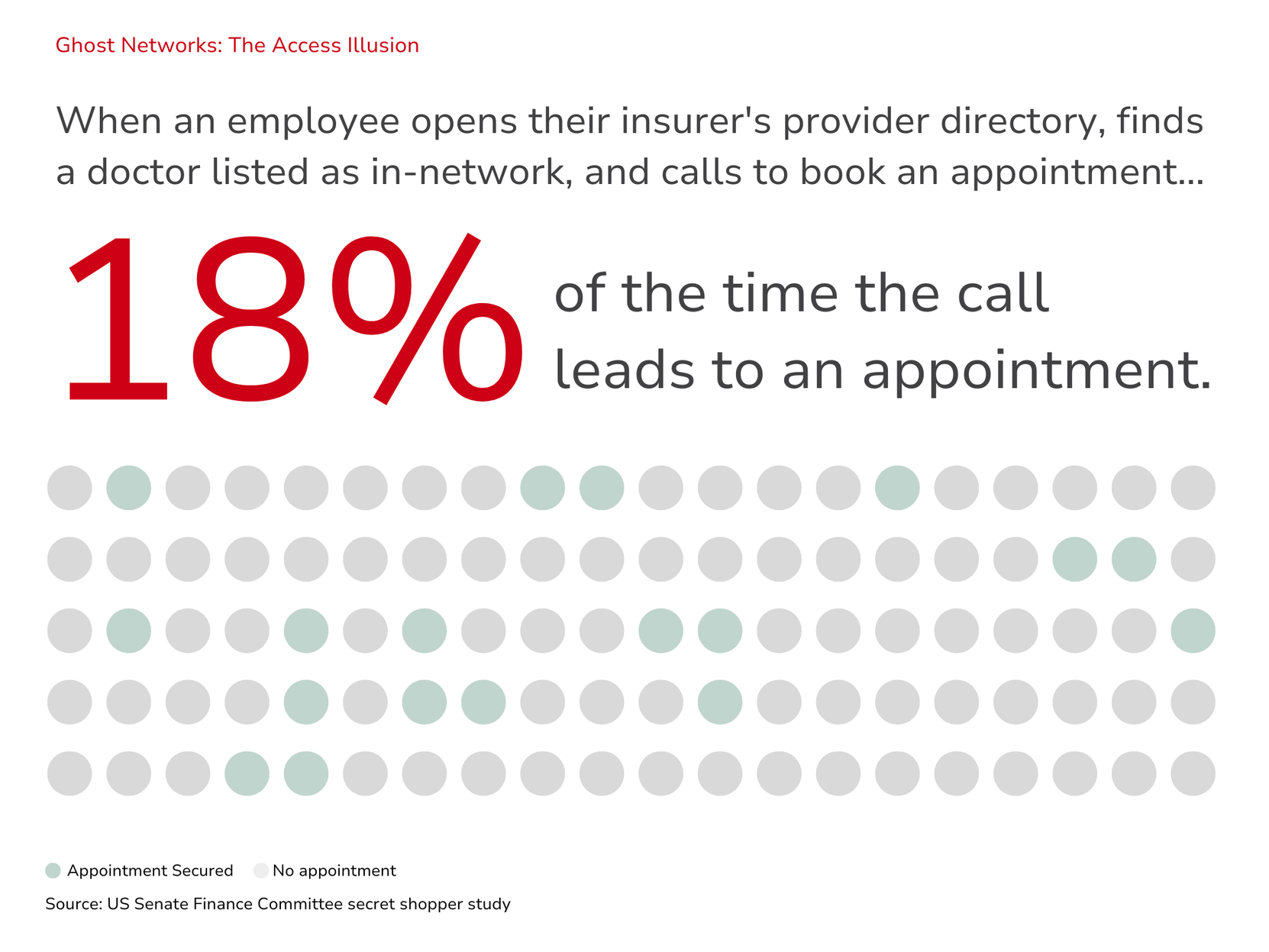
A study published by JAMA Open Network found that 81% of entries across provider directories of five large insurers contained inaccuracies. A secret shopper study conducted by the US Senate Finance Committee found that appointments could only be secured 18% of the time when contacting providers listed in network directories.
The practical implication here is significant. Employers may believe their workforce has access to a robust network of providers. In many cases, that access exists on paper more than in practice. When directory data cannot be trusted, the access argument for networks weakens considerably. Employees encounter friction when seeking care, face unexpected out-of-network costs, or simply give up on finding a listed provider. Ultimately, the network that was supposed to simplify access often complicates it.
The default became the strategy
None of this means PPO networks have no value. For many employers, particularly those with geographically dispersed workforces, a broad network still serves an important administrative function. Networks are not the enemy. But they are also not a strategy on their own.
The problem is how networks came to be treated. Over decades, the PPO became the default option in employer benefits. Advisors presented it. Carriers promoted it. Employers accepted it. And with repetition, the default became indistinguishable from the strategy. Choosing a network felt like making a strategic decision because it was the most visible decision available. But selecting a network is an infrastructure choice, not a strategic one. It determines which providers are covered. It does not determine whether those providers are delivering care at fair prices, whether the funding structure makes sense for the employer, or whether the plan design is aligned with the actual health needs of the workforce.
Strategy happens before the network selection. It starts with questions about employer goals, cost tolerance, workforce demographics, and risk appetite. The network is one tool that may or may not be the right fit depending on the answers to those questions. When that sequence gets reversed—when the network comes first and everything else is built around it—the strategy is inherited, not designed.
What employers are beginning to ask
The sustained rise in healthcare costs is pushing more employers to examine the assumptions behind their benefit strategies. Many are starting to ask not just which network, but whether a traditional network structure is the right foundation at all.
This shift is producing real interest in approaches that start from different premises: direct provider contracting, reference-based pricing, self-funded structures, and alternative funding models that prioritize pricing transparency over network discounts. These are not fringe ideas. They represent a growing segment of employer benefits strategy, particularly among mid-size and smaller employers who have more flexibility and more urgency to find approaches that actually control cost.
The common thread in all of them is that they treat the network as one possible tool rather than the automatic starting point. They begin with strategy and work toward structure—not the other way around.
The bottom line
Networks were built to manage access. In many cases, they still do that. But the industry’s habit of treating network selection as a proxy for benefits strategy has produced a generation of plans that are designed around infrastructure rather than outcomes.
When employers begin to separate the access question from the cost question, the conversation about benefits changes. The network stops being the default answer and starts being one option among several—evaluated on its actual merits rather than its institutional familiarity.
That shift in thinking is where smarter benefit design begins. And it raises a question that goes beyond the network entirely: if the annual renewal cycle has been built around a structure that was never designed to control costs, what does it mean to actually design a benefits strategy from scratch?
Look for a discussion on designing benefits strategy in our next blog.
Ready to stop fighting an outdated system and start building benefits that work?
Explore
SUGGESTED FOR YOU


